
Speaker
 Erik J. Nuveen, MD, DMD, FAACS
Erik J. Nuveen, MD, DMD, FAACS
Cosmetic Surgery Affiliates, Oklahoma City, OK
Dr. Nuveen has performed exclusively cosmetic surgery his entire 19-year career. He has been a member of the AACS since 2000. He has performed more than 19,000 major surgeries and written 21 first author articles and 9 textbook chapters on all aspects of cosmetic surgery. He is director of fellowship and has trained more than 15 fellows. His practice is located in Oklahoma City and treats patients from throughout the world.
Abstract
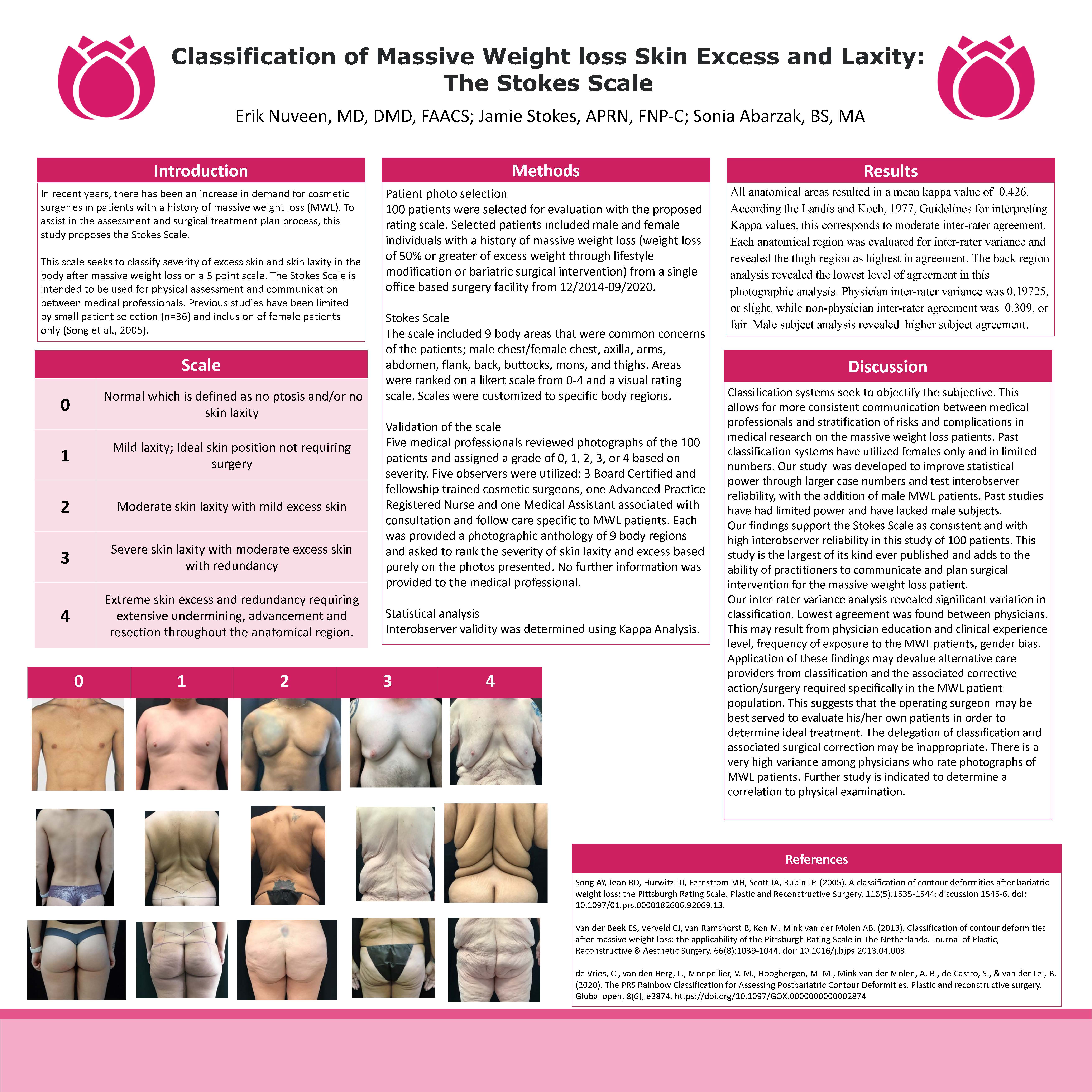
Background: In recent years, there has been an increase in demand for cosmetic surgeries in patients with a history of massive weight loss (MWL). To assist in the assessment and surgical treatment plan process, this study proposes the Stokes Scale. This scale seeks to classify severity of excess skin and skin laxity in the body after massive weight loss on a 5-point scale. The Stokes Scale is intended to be used for physical assessment and communication between medical professionals. Previous studies have been limited by small patient selection (n=36) and inclusion of female patients only.
Methods: 100 patients were selected for evaluation with the proposed rating scale. Selected patients included male and female individuals with a history of massive weight loss (weight loss of 50% or greater of excess weight through lifestyle modification or bariatric surgical intervention) from a single office-based surgery facility from 12/2014-09/2020. The scale included 9 body areas that were common concerns of the patients: male chest, female chest, axilla, arms, abdomen, flank, back, buttocks, mons, and thighs. Six medical professionals reviewed photographs of the 100 patients and assigned a grade of 0, 1, 2, 3, or 4 based on severity.
Discussion: Classification systems seek to objectify the subjective. This allows for more consistent communication between medical professionals and stratification of risks and complications in medical research on the massive weight loss patients. Past classification systems have utilized females only and in limited numbers. Our study was developed to improve statistical power through larger case numbers and test interobserver reliability, with the addition of male MWL patients. Past studies have had limited power and have lacked male subjects. 6 observers were utilized: 3 Board Certified and fellowship trained cosmetic surgeons, one fellow in training, one Advanced Practice Registered Nurse and one Medical Assistant associated with consultation and follow care specific to MWL patients. Each was provided a photographic anthology of 9 body regions and asked to rank the severity of skin laxity and excess based purely on the photos presented. No further information was provided to the medical professional. A scale of severity was provided as:
0: No laxity
1: Mild laxity; Ideal skin position not requiring surgery
2: Moderate skin laxity with mild excess skin
3: Severe skin laxity with moderate excess skin with redundancy
4: Extreme skin excess and redundancy requiring extensive undermining, advancement and resection throughout the anatomical region.
Our findings support the Stokes Scale as consistent and with high interobserver reliability in this study of 100 patients. This study is the largest of its kind ever published and adds to the ability of practitioners to communicate and plan surgical intervention for the massive weight loss patient.
Take Home Message
The MWL population has extreme variation in severity of skin excess and laxity. Our classification system was developed to more objectively stratify the wide range of complexity in body contour as a result of MWL. This classification should be use in communication with other medical providers, insurance carriers and patients to enhance diagnosis and associated treatment planning.